Cervical Cancer
Learn about cervical cancer
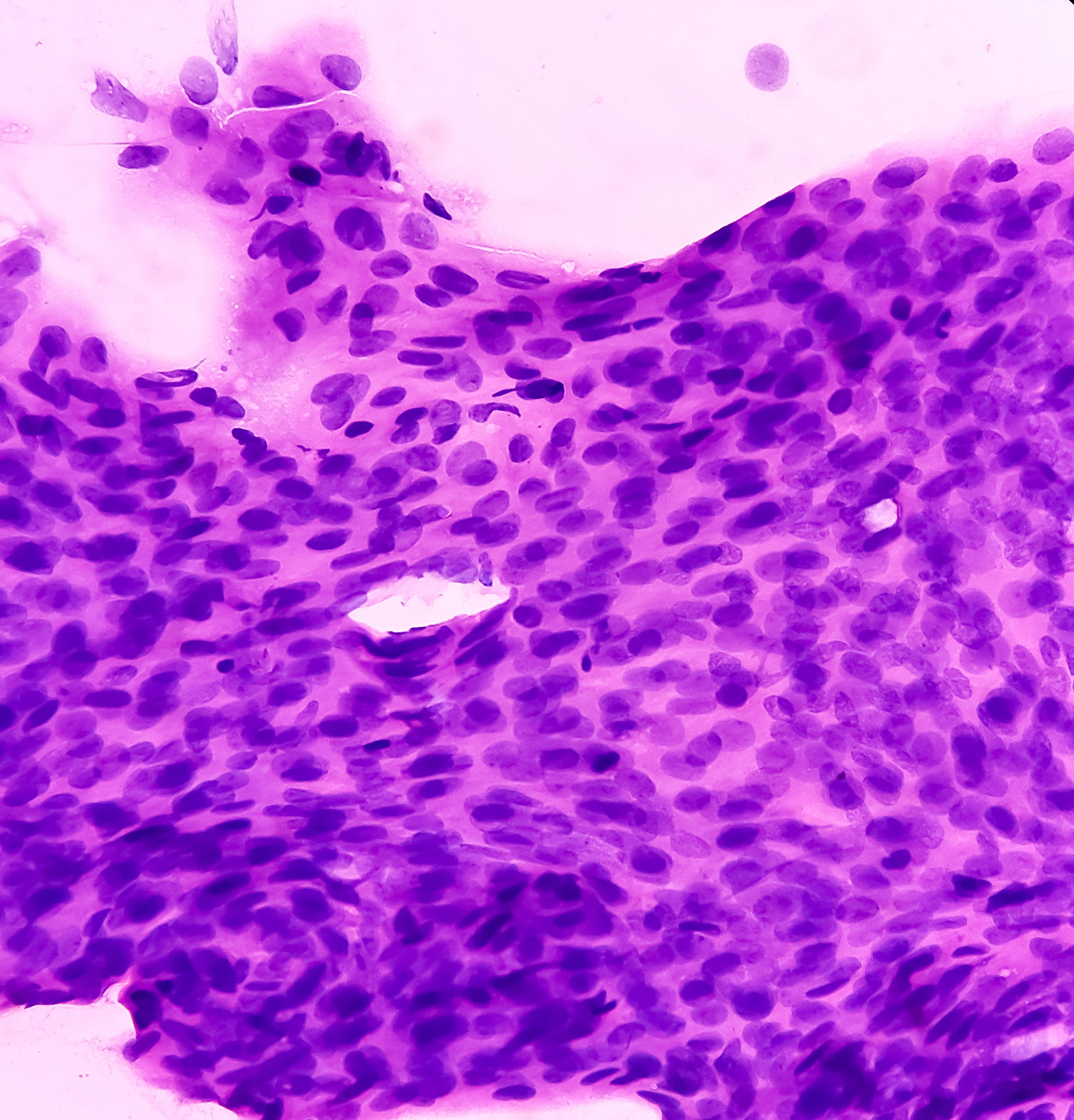
Cervical cancer arises from the tissues of the cervix– the opening of the uterus extending into the upper end of the vagina. It usually grows slowly, over many years.
The cervix is covered by two kinds of cells: squamous and glandular. The squamous cells are flat, thin cells found in the outer layer of the cervix. The glandular cells are found in the cervical canal.
Before true cancer cells develop, the cervix tissues undergo changes called dysplasmia, or pre-cancers, which can be detected in a pap test. If left untreated, these pre-cancers can become cancerous.
The two main types of cervical cancer are:
- Squamous cell carcinoma: This is the most common type of cervical cancer, accounting for 80 percent of all cases. It starts in the squamous or skin-like cells of the cervix.
- Adenocarcinoma is less common and develops in the glandular cells. This kind of cervical cancer is more difficult to diagnose as it begins higher up in the cervix and is harder to reach with the brush used during a pap smear.
Cervical cancer can be micro-invasive or invasive:
- Micro-invasive cancer occurs when cancer cells have broken through the boundary between the surface of the cervix and the underlying tissue. At this stage, the cells have not spread more than five millimetres into the tissues of the cervix.
- Invasive cervical cancer is when cancer cells have spread into the underlying tissue of the cervix to a depth of more than five millimetres. The cancer may also have spread to the vagina, the lymph nodes, other tissues surrounding the cervix, or into nearby organs such as the bladder or rectum.
Pre-cancerous stages of cervical cancer rarely show any signs. If these abnormal cells do become cancerous the most common symptoms include:
- Vaginal bleeding between periods
- Menstrual bleeding that is unusually long or heavy
- Bleeding after intercourse
- Pain during intercourse
- Vaginal discharge that is unusual
- Vaginal bleeding after menopause
- Excessive tiredness
- Leg pain or swelling
- Lower back pain
If any of these symptoms arise it is best to speak with a GP.
A pap test will detect early cell changes in the cervix which could potentially develop into cervical cancer. There are different types of early cell changes:
- Atypia: The cervical cells have changed slightly. The cells may return to normal by themselves or the changes may worsen. If a cell shows signs of atypia, it doesn’t necessarily mean you have cancer or will get cancer. Atypia can also be caused by infection or irritation.
- Squamous abnormalities: This may be classified as a low-grade or a high-grade abnormality on a pap test. High-grade abnormalities are pre-cancerous, and although they don’t usually cause symptoms they can sometimes progress to early cervical cancer if they’re not detected and treated properly.
If a pap test does come back as abnormal then your doctor will recommend one of these actions:
- Another pap test in 12 months’ time to monitor the cells.
- A biopsy.
- Immediate treatment.
Diagnosing cervical cancer
If a pap smear does detect changes, more tests and possibly treatment will be needed. Doctors may advise some or all of the following to confirm diagnosis:
- Colposcopy: allows the doctor to see a magnified view of the cervix, vagina and vulva to help identify where abnormal or changed cells are located and what they look like.
- Cone biopsy: Determines if the abnormal cells have spread to tissue beneath the surface of the cervix. A cone biopsy is also used to treat very early and very small tumours.
- Large loop excision: Removes a large sample of the cervix for examination.
After cervical cancer is diagnosed, one or more of the following tests are used to determine the extent and severity of the cancer (its stage):
- Blood tests
- Examination under anaesthetic
- Chest x-ray
- CT scan
- MRI
- PET scan
Once the stage is determined the most appropriate treatment can be discussed.
Treating cervical cancer
For small pre-invasive tumours found within the cervix, surgery is the most common treatment. If the tumour is very small a cone biopsy may be advised to surgically remove the cone-shaped tissue containing the cancer.
Laser surgery, which uses a narrow beam of intense light to kill the cancerous cells, is another option.
Loop excision, in which an electrical current is passed through a thin wire loop to remove the cells may also be used.
If the tumour is more developed, a total or radical hysterectomy, involving the surgical removal of the uterus, may be required.
Radiotherapy, which uses x-rays to kill or injure cancer cells so they cannot multiply, and chemotherapy, which uses drugs to kill or slow their growth, are often combined to make treatment of this disease more effective.
Long term infection with certain types of the Human Papilloma Virus (HPV) is now known to be the cause of almost all cervical cancers. Almost all abnormal pap test results are caused by HPV.
HPV is commonly spread by sexual contact as many people may not be aware of any signs or symptoms. HPV does not always lead to cervical cancer. However, if the virus persists and is left undetected, the viral cells can become cancerous.
In 2006, Professor Ian Frazer and his team at the University of Queensland discovered a vaccine to prevent HPV, protecting women against most types of cervical cancer.
Recently it was reported that there has been an incredible 93% drop in genital wart diagnoses (symptoms of the human papillomavirus) in young women who have received the HPV, or cervical cancer, vaccine since 2007.
The vaccine has also begun to be administered to young males as it has been found to help prevent cancers of the genital tract, some types of head and neck cancers, and it will also enhance the vaccine’s effectiveness in women.
The research was kick-started with an ACRF grant in 1999.